Helping rural health care providers cope with pandemic stress
Caring for the caregivers
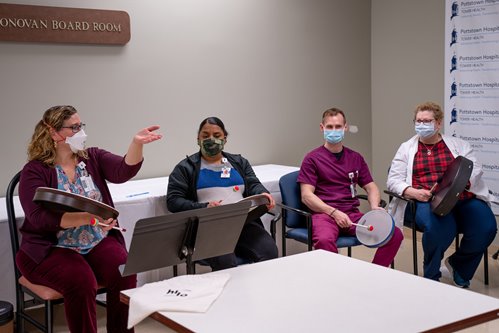
When she’s in the drum circle, Donna Martz feels like she can breathe. As ICU director at Pottstown Hospital — Tower Health in Pottstown, Pa., Martz, MSN, RN, CCRN, has been caring for her community’s sickest COVID-19 patients for more than two years. Like many health care providers, she is passionate about her work, but the stresses of the pandemic combined with staffing shortages and working long hours have taken a toll on her well-being. Responding to COVID has led Martz and her team to experience fear and anxiety — and, in some cases, anger.
“At the beginning, we were all afraid because we didn’t know anything about this,” says Martz, who has worked as a nurse for 40 years. “Are we going to catch this? Are we going to take it home to our families? We had a lot of sadness because a lot of people died, and many of them were young. During the second phase, I think anger was one thing we all felt, because we were seeing patients who were not vaccinated. With what we’ve seen, we couldn’t wrap our heads around why people would not get vaccinated. It has affected people very strongly.”
To help Martz and other providers cope with stress and other symptoms of burnout, Pottstown Hospital began offering a music therapy program for frontline employees this winter through an innovative statewide partnership. Utilizing grant funding from the Pennsylvania Council on the Arts, which aims to strengthen the cultural, educational, and economic vitality of Pennsylvania communities, the Hospital and Healthsystem Association of Pennsylvania (HAP) is helping hospitals implement music therapy programs for health care providers at eligible facilities across the state, including both urban and rural areas.

Using music to address trauma
A membership-based nonprofit, HAP works with hospitals and health systems to improve the health and well-being of Pennsylvanians. This mission positioned their organization to take the lead in the Music Therapy Collaborative, which is being rolled out to HAP’s members in three phases and allows facilities to work directly with board-certified music therapists to design programs based on their unique needs. The initiative is part of the organization’s broader, pre- COVID goal to address health care worker wellness, support resiliency, and offer resources to their members.
“The Music Therapy Collaborative targets mainly frontline workers who work directly with patients. It is an opportunity to provide respite to clinicians,” says Mary Marshall, HAP senior director of workforce and professional development. “It’s about caring for our caregivers and giving them the chance to express their emotions.”
Because HAP’s program is one of the nation’s first using the creative arts to address clinician burnout on a statewide scale, many hospital workers are being introduced to music therapy for the first time. It is widely accepted that music can impact mood, but music therapy involves much more than the good vibes people get from listening to their favorite songs. In fact, it is a clinical and evidence-based intervention conducted by a credentialed professional, and it is increasingly recognized as an effective tool to combat a variety of mental health and wellness challenges.
“Specific to health care, music therapy has been shown to be an effective, non-pharmacological, economical, and non-invasive means of significantly decreasing stress levels and addressing trauma,” says Norah Johnson, Pennsylvania Council on the Arts director of external affairs and public awareness. “Music therapy has been proven to be a valuable tool for health care workers experiencing compassion fatigue and burnout.”
As for the typical session, Marshall likens it to a variation on traditional counseling. A music therapist works with attendees either individually or in a group, giving them a safe place to process and express their feelings through activities such as playing an instrument, writing song lyrics, or participating in a drum circle. This type of emotional release has been enormously beneficial for overwhelmed health care providers.
"Most people in health care feel like they’ve been called to do their work — they feel like it’s what they’re meant to do. They’re the people running into the fire instead of running out of the fire. That’s their very nature …"
- Julie Carr, RN, MSN
For Martz and other Tower Health staff, the effect of attending regular music therapy sessions has been immediate and profound.
“Some people smile the whole time, some close their eyes, some cry,” she says. “You’re away from that stressful environment for 15 or 20 minutes, and the difference that makes is indescribable. For me, I think it’s a tension reliever. I’m here to support the staff as much as I can and care for patients who are very sick — so for me it’s a sigh of relief. I can have nice deep breaths and relax.”

‘All boots on the ground’
A big factor contributing to rural health care worker burnout is the all-encompassing job of responding to the pandemic with resources that are already stretched thin. At NRHA member Roane General Hospital in Spencer, W.Va., the facility was in the midst of a renovation and expansion when COVID hit. During the pandemic, Roane General started providing oncology and wound care and added specialists to their rural health clinic while simultaneously caring and doing case management for COVID patients, including running vaccine and monoclonal antibody clinics.
“Our primary focus had to become COVID and the pandemic, but we were still trying to move toward services that we believe are imperative for our community,” says Julie Carr, RN, MSN, Roane General chief clinical officer. “While we were dealing with COVID we were trying to fulfill the original mission of our hospital — providing services close to home — and our renovation project. All of this we were trying to manage at the same time with limited resources.” Compounding the problem, West Virginia’s EMS system is chronically overwhelmed and resources in surrounding communities are also taxed, leaving Roane General without their usual plan of action when treating critical patients, who are typically transferred to tertiary facilities. At times during the pandemic, no ICU beds were available in West Virginia or surrounding states — Carr says they have called up to 40 facilities at a time to find space, having transported patients as far away as Tennessee. This has left Roane General treating critical patients they might not typically see.
"We’ve never been off for 24 months. We might not be clocked in, but we’re never away from COVID…"
- Julie Carr, RN, MSN
While Carr is proud of what her facility and staff have been able to accomplish during the pandemic in terms of meeting strategic goals and continuing to offer high-quality patient care, she recognizes that it has come at a cost. In addition to media campaigns and giveaways to support providers, Roane General has bolstered mental health resources by providing counselors and therapists to help frontline staff deal with stress. Carr also notes that in a rural community, the pandemic hits differently.
“We’re highly integrated in our community — the person we are taking care of could have been our teacher or someone we go to church with,” she says. “It’s a different type of connection. People are living with scenarios like that internally, and that comes to light in day-to-day work efforts through burnout or leaving the profession. You’re never really at rest from it — it’s always there, and you always have to be connected to what’s going on with COVID. We’ve never been off for 24 months. We might not be clocked in, but we’re never away from COVID, and that is a mentally stressful situation.”
.jpg?width=921&ext=.jpg "DSC04072-(1).jpg")
Recognizing and responding to burnout
Identifying and responding to burnout is so vital because the consequences of ignoring it can be devastating for providers and patients alike. Yalda Jabbarpour, MD, is a family physician and medical director of the Robert Graham Center for Policy Studies in primary care, where she helps create and curate evidence to inform primary care policy. She studies factors that predispose family physicians to burnout as well as what can help mitigate this concern, and she presented on this topic at NRHA’s Rural Health Policy Institute in February.
“Like in other professionals, burnout is typically defined by two phenomena: emotional exhaustion and depersonalization or callousness,” Jabbarpour says. “For physicians this may look like anything from being less engaged with patients or their staff to the absolute worst scenario — making errors in patient care or management because they are so exhausted. Burnout is a systems issue, not an individual one. It is contingent upon medical organizations that employ physicians to set up environments that prevent burnout.”
To achieve this goal, Jabbarpour has a bold proposal: Change the health care system. This includes moving away from a fee-forservice model, setting up social safety nets that allow vulnerable populations to have their social determinants of health needs met, providing flexibility in work schedules, allowing health care workers more autonomy in how and when patients are seen, and creating a culture that puts health care workers and patients first.
“Of utmost importance is creating environments where physicians have the autonomy to do what they are meant to do — take care of their patients,” she adds.
In Pennsylvania, HAP’s music therapy collaborative represents this type of a cultural shift toward a focus on wellness, and Tower Health’s Martz hopes to continue offering it once grant funding ends. Meanwhile, in West Virginia, Roane General leaders are studying why so many nurses are leaving the profession. They are also looking at new ways to support providers, such as developing peer support programs and creating a proactive pandemic response plan. According to Roane General’s Carr, the overarching sentiment is simple: Health care workers have a vital job to do, but they can’t do it without support — and a little gratitude goes a long way.
“Most people in health care feel like they’ve been called to do their work — they feel like it’s what they’re meant to do,” Carr says. “They’re the people running into the fire instead of running out of the fire. That’s their very nature. I’m very appreciative of what our entire hospital has been able to do for our community, but it’s not without challenges for all of us. I think it’s important to say thank you to health care workers any opportunity we get.”